|
Cruciate ligament rupture |
|
 |
|
The most common cruciate ligament injuries (Cruciate ligament rupture) are caused by training errors |
|
|
|
|
Training and rehabilitation of the knee, so that it works like a well-oiled machine
The prerequisite for the restoration of a painless, stable knee joint is the functional anatomy, the functioning joint structure. The shape of the articular surface, the density of the bone, the elasticity of the cartilage, the size and strength of the ligaments and muscles acting on the joint are indicative of adaptive responses to exertion.
The roll-glide principle, i.e. a combination of turning and moving, must be considered to understand knee joint structure-function. The central stabilizing pillars are the anterior and posterior cruciate ligaments (CL). Both have virtually no blood supply, pass through a cavity and when completely torn can no longer grow together. The CL, in particular the anterior CL, is today routinely operated upon arthroscopically, i.e. with a so-called mini surgical operation. The procedure is significantly simpler than earlier conventional open surgery. The surgical risk is moreover very small. If however the tear is incomplete and some fibres are intact the ligament can regenerate itself along these fibres without surgery. The lateral ligaments are surrounded by structures that are well-perfused with blood and can be healed by conservative therapy. Surgery is rarely necessary. Ruptures of the crescent-shaped, cartilaginous wedges of the inner and outer menisci can be restored arthroscopically and can thus be repaired with relatively little surgical effort.
Although the orthopedic and trauma surgical treatment of CL rupture has improved significantly, the problem still remains that, even with optimal care, the incidence of osteoarthrosis, i.e. cartilage damage caused by injury and/or by the operative procedure, is very high. Preventive measures and rehabilitation are thus especially important, i.e. training and rebuilding of the cartilage structure. The symptoms of pain, and swelling and to some extent restricted movement, can be well managed by physiotherapy, electrotherapy, lymphatic drainage, natural medicines such as devil's claw, coral calcium and rose hip powder and pharmaceutical drugs. For cartilaginous regeneration, the natural substances chondroitin and glucosamine, which are offered as nutritional supplements and have been demonstrated to improve the development and the sliding properties of articular cartilage, are available. Hyaluronic acid can be introduced into the joint by injection because it acts both as a lubricant and water retainer.
The most important measure to improve stability and prevent wear and tear, i.e. osteoarthrosis, is the exercise program to stretch the shortened muscles and to strengthen the stabilizing muscles as well as the correction and improvement of the movement program. Errors made in gyms, and during sports and fitness training are a particular problem. The roll-glide principle of the knee makes it particularly vulnerable to injuries that are caused by unilateral thigh muscle training. The person with the thickest and strongest thigh doesnt have the most stable knee joint, rather the one with an exercise program that provides optimal control of the muscles.
The more abrupt and uncontrolled the pulling of the anterior thigh muscles over the kneecap is, the greater the strain on and risk of rupture of the anterior CL. Every forced extension leads to the pushing forward of the lower leg (drawer phenomenon) which is held in check by the anterior CL. It is thus possible to injure the CL with a particularly strong quadriceps (muscle at the front of the thigh). Many patients and athletes therefore report, when asked precisely, that they felt the tear in the knee before falling. I know of athletes who have torn the anterior CL by only a sudden movement, a stop step, a compression against a bump, etc. i.e. without falling. The increasing incidence of these isolated CL ruptures can be attributed to unilateral strength training. The main danger lies in maximal strength training of the thigh muscles
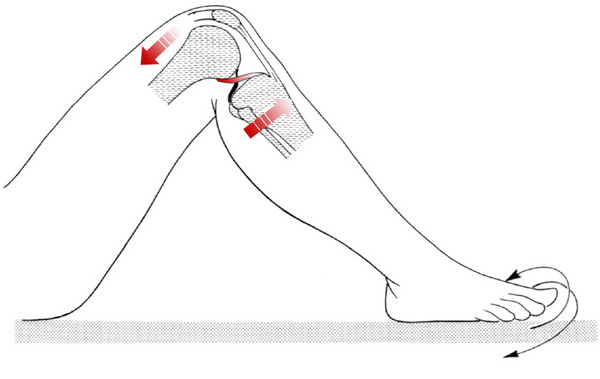
Picture 1: Isolated training of the quadriceps damages the anterior CL through forward displacement of the lower leg. The displacement of the joint surfaces increases with increased rotation of the joint (CL rupture/ CL injuries
 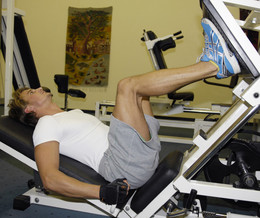 
Pictures 2, 3, 4: Training the thighs with flexed hips and a hollow back causes the quadriceps at the front of the thighs to act extremely strongly on the knee joint and to damage it. The stretching movements cause the displacement of the joint surfaces with respect to each other and the overloading of the anterior CL. An abrupt tensing of a highly trained muscle can injure the knee and cause a torn CL.
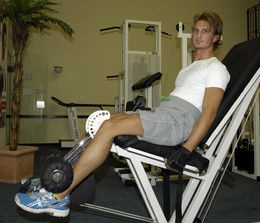
Figure 5: Athlete in the gym
We therefore recommend that you start training without equipment or only under precise supervision
|
|
|
|
|
|
|
|